An inherited cholesterol risk turns up in 1 in 6 Ultrahuman members, and a normal LDL hides most of it
Across 2,452 members, 1 in 6 had elevated lipoprotein(a), an inherited risk a standard cholesterol test misses, and for 59 percent of them the LDL on the same panel read normal.
A standard cholesterol panel reports the cholesterol packed inside your LDL particles, but it cannot see whether those particles carry an extra, genetically fixed protein tail. Lipoprotein(a), or Lp(a), is the LDL-like particle that does. Its blood level is set largely by the LPA gene, stable from childhood, and barely shifts with diet, exercise, or statins. In 2024 the National Lipid Association moved Lp(a) into its once-in-a-lifetime universal-screening recommendation, with the elevated-risk cut-off at 50 mg/dL (or 125 nmol/L) and very-high at 100 mg/dL (250 nmol/L) (Koschinsky et al., 2024). Two findings drove the shift. A UK Biobank cohort of 460,544 adults followed a median 13.6 years reported a hazard ratio (the relative rate of a new event per unit of exposure) near 1.18 per 75 nmol/L of Lp(a) for incident peripheral artery disease and 1.17 for carotid disease, adjusted for standard lipids (Bellomo et al., 2025). The phase-2 ALPACA trial of lepodisiran, a small interfering RNA that silences LPA messenger RNA, reduced serum Lp(a) by 93.9 percentage points versus placebo at the 400 mg dose, with the effect persisting through 360 days (Nissen et al., 2025). The screening case turns on one question: how often does an Lp(a) test surface something a standard panel does not?
We took the most recent Blood Vision panel carrying an Lp(a) value for each member between August 2025 and April 2026, excluded ambiguous below-detection-limit readings, and applied the NLA thresholds to the 2,452 members left. For the 2,231 whose same panel also reported LDL, we called it normal or elevated against the ACC/AHA 2018 cut-off of 130 mg/dL.
Across 2,452 members, the test flags risk a routine panel cannot. 397 (16.2 percent, 95 percent CI 14.8 to 17.7) carried elevated Lp(a), and 71 (2.9 percent) sat in the very-high band. Within the 2,231 with a paired LDL, the standout cell is elevated Lp(a) sitting behind a normal LDL: 213 members, or 9.5 percent of the subset.
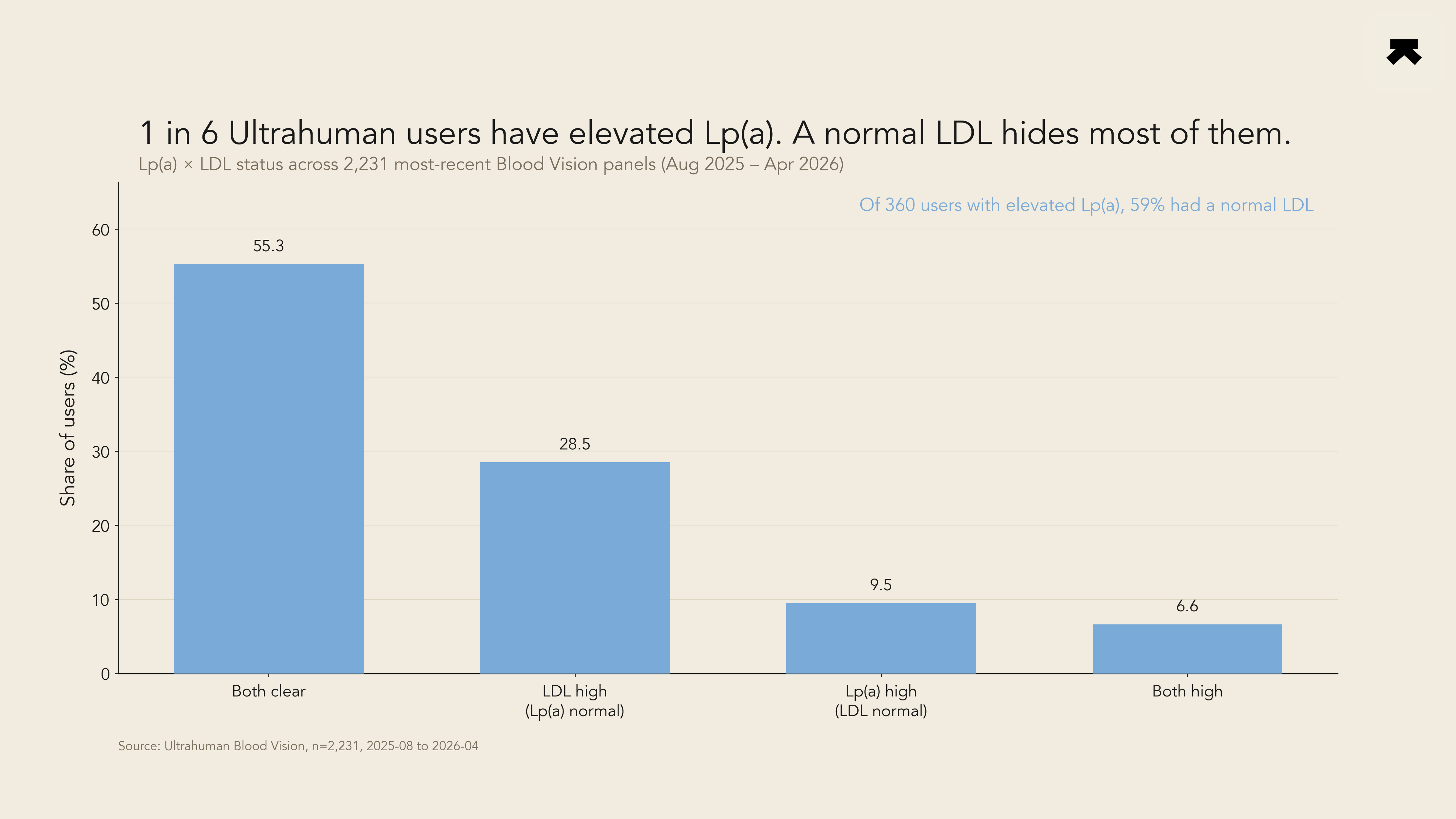
Figure 1. Distribution of 2,231 Ultrahuman Blood Vision panels across the four LDL by Lp(a) quadrants. Cut-points: LDL 130 mg/dL (ACC/AHA 2018); Lp(a) 50 mg/dL or 125 nmol/L per the 2024 NLA scientific statement, applied unit-matched. Concordant-low (LDL and Lp(a) both normal) 55.3 percent; LDL-only elevated 28.5 percent; hidden Lp(a) (LDL normal, Lp(a) elevated) 9.5 percent; both elevated 6.6 percent.
The answer is roughly three in five. Of the 360 members with elevated Lp(a) and a paired LDL, 213 (59.2 percent) had a normal LDL, so a routine report would have cleared most of them. Prevalence held flat across age, as a genetic marker should: 16.2 percent at 18 to 34 (n = 1,004), 15.7 percent at 35 to 49 (n = 1,069), and 16.8 percent at 50 and over (n = 310), within 1.1 percentage points. A second marker did not rescue the missed cases. Among the 1,931 members with Lp(a), LDL, and ApoB on one panel, 105 (5.4 percent, 95 percent CI 4.5 to 6.5) carried elevated Lp(a) while LDL stayed below 130 mg/dL and apolipoprotein B (ApoB), the count of all atherogenic particles, below 90 mg/dL. The Lp(a)-versus-ApoB contrast deserves its own analysis; this cross-sectional design describes prevalence, not cardiovascular outcomes.
One in six Ultrahuman members carries an inherited cardiovascular risk their LDL alone does not reveal, and for most of them a standard cholesterol report reads clean. The level is genetically set and barely moves over a lifetime, so a single test tells you where you stand and lets you manage the rest of your risk accordingly. On this evidence, the case for adding Lp(a) to a routine panel is hard to argue against.
More bytes
Keep exploring

Across 230,179 Ring members, the dominant age change in sleep is more time awake at night, not less deep sleep

Time in target holds until the diabetic line, then collapses, across 1,169 members
