Short sleep costs overnight recovery more than long sleep does, across 229,837 Ring members
Across 229,837 Ring members, overnight HRV, resting heart rate, and the Ring’s recovery score all sit best at 7 to 9 hours of sleep. The cost of under 6 hours is steep; past 9 hours it is small.
The population sleep-duration mortality curve is settled. A 16-study meta-analysis of 1,382,999 participants found all-cause mortality U-shaped in habitual sleep, with relative risk (the mortality ratio between groups) of 1.12 in short sleepers and 1.30 in long sleepers against 7-to-8-hour sleepers (Cappuccio et al., 2010). A companion meta-analysis of 474,684 participants carried the same U into cardiovascular outcomes (Cappuccio et al., 2011), and the consensus that followed lands on 7 to 9 hours for healthy adults (Hirshkowitz et al., 2015). What that work cannot reach is whether the U shows up in the night-by-night recovery state of healthy adults, on the overnight reading a consumer Ring captures.
We took every Ultrahuman Ring member with at least 30 valid main-sleep nights in the 120 days from 25 December 2025 to 24 April 2026 whose profile recorded age and gender: 229,837 members, a mean of 78 nights each. We sorted each by typical nightly sleep into the five National Sleep Foundation bands and read three overnight markers: heart-rate variability (HRV), a reading of how rested the nervous system is; resting heart rate; and the Ring’s composite Dynamic Recovery score.
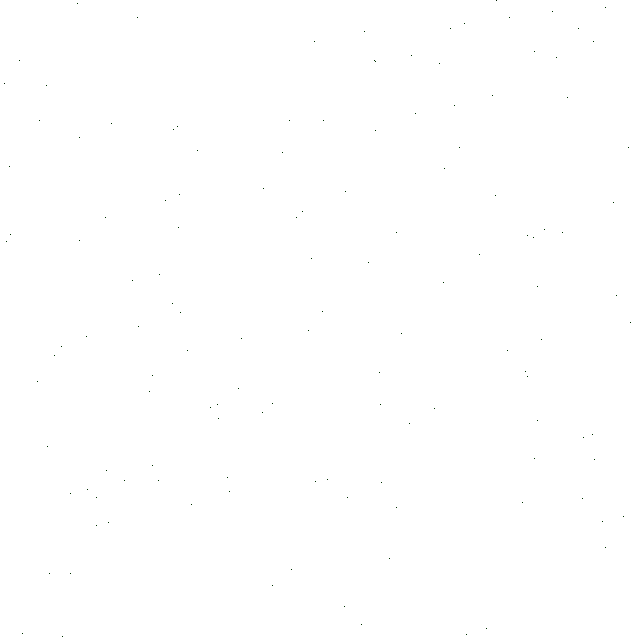
All three markers land in their best zone between 7 and 9 hours, and the short end costs far more than the long end. Overnight HRV peaks at 44.0 ms at 8 to 9 hours, falling to 41.3 ms below 6 hours and 42.4 ms above 9 hours. Overnight resting heart rate bottoms at 56.6 bpm in the same band, rising 3.0 bpm at the short end and only 1.0 bpm at the long end. The composite Dynamic Recovery score climbs 17.6 points from the short end to the peak, then stops improving.
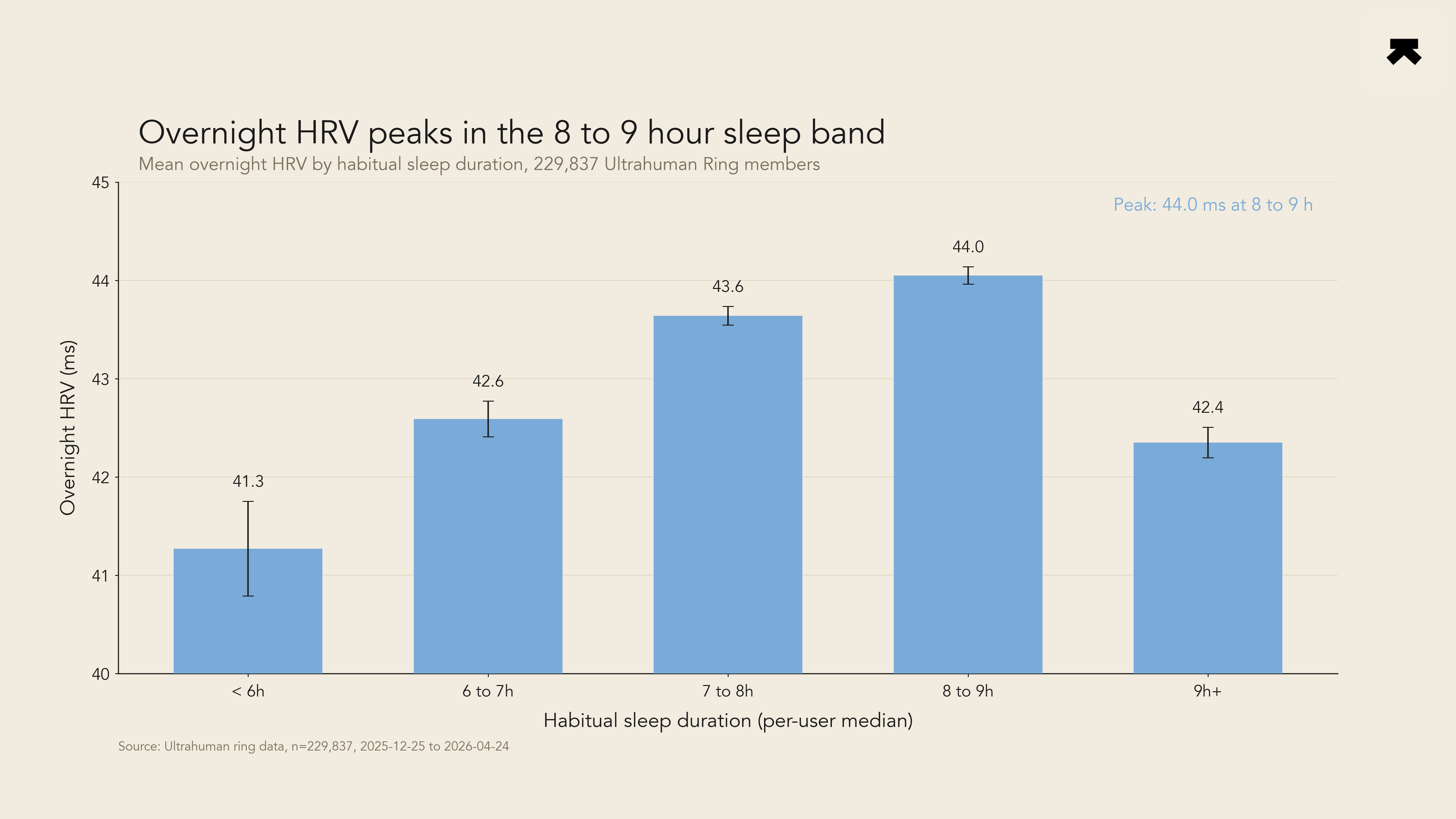
Figure 1. Mean overnight HRV (ms) by habitual sleep-duration band, in 229,837 Ultrahuman Ring members with at least 30 valid main-sleep nights in the 120-day window ending 24 April 2026. Bands follow the National Sleep Foundation ranges. Error bars are 95 percent normal-approximation confidence intervals.
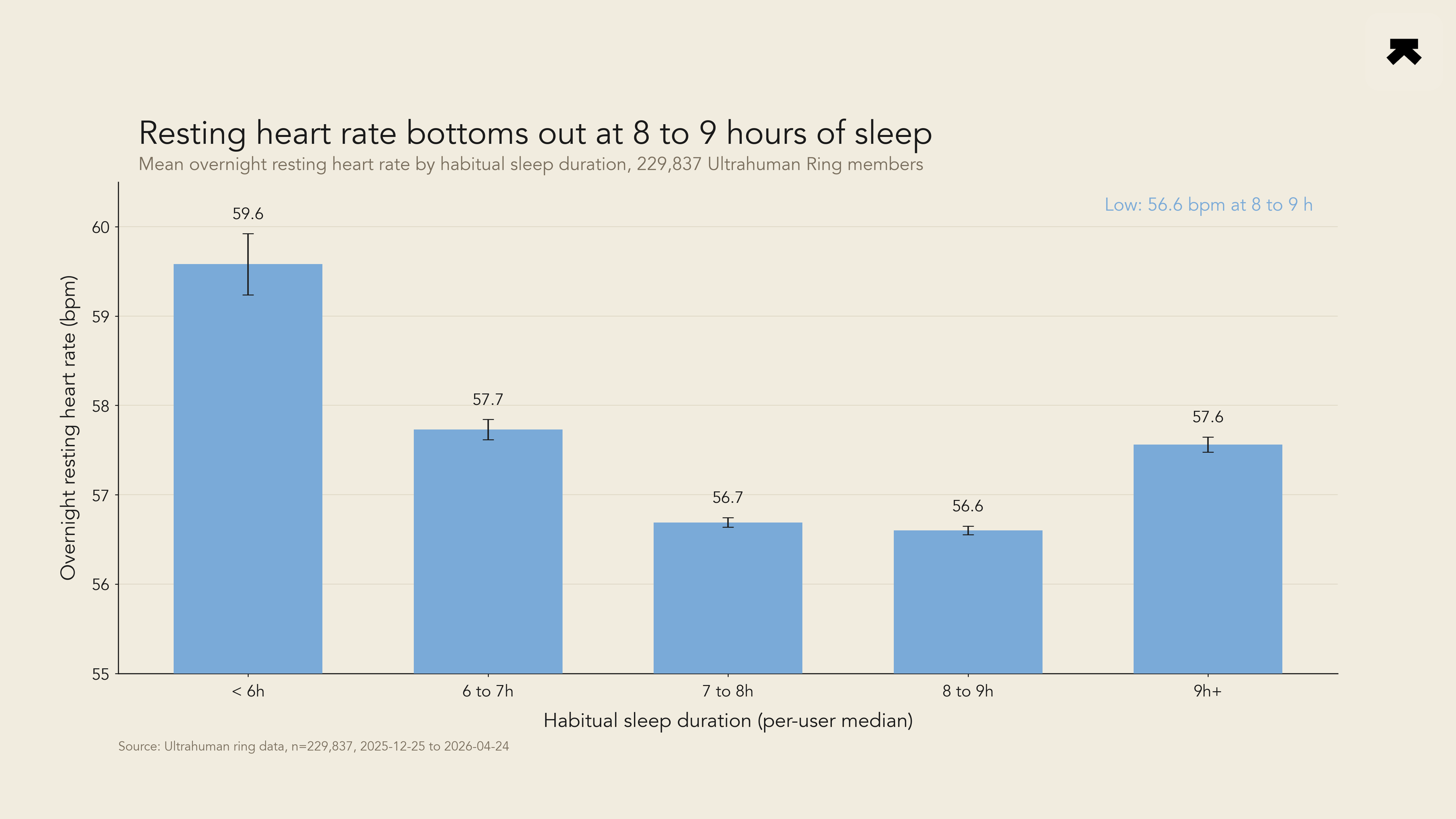
Figure 2. Mean overnight resting heart rate (bpm) by the same habitual sleep-duration band and cohort as Figure 1. The HRV peak and the resting-heart-rate trough both fall at 8 to 9 hours.
Figure 3. Mean Ring Dynamic Recovery score (0 to 100) by the same habitual sleep-duration band and cohort. The dose-response saturates rather than inverting at the long-sleep end.
HRV peaked where the literature predicts and resting heart rate troughed in the same band, but the composite climbed and then flattened rather than turning back down, and that is where the three markers disagree. The composite rose from 58.0 below 6 hours to 75.6 at 8 to 9 hours, a 17.6-point gap (Cohen’s d, a standardised effect size where 0.2 is small and 0.8 is large, of 2.19), then held at 75.2 past 9 hours (d = 0.07). HRV does not flatten: its long arm dips 1.7 ms off the 44.0 ms peak (d = 0.12), small but cleanly separated from zero at this cohort size. The composite reading is partly circular here, since the Dynamic Recovery score takes sleep duration as one of its inputs alongside HRV and resting heart rate, so the independent overnight markers carry the weight of the read. The reading is that the population long-sleep mortality tail (relative risk 1.30) carries a large component of unmeasured illness, since ill people sleep more, so in a healthier cohort the long arm survives only on the most sensitive marker. A time-window split moved every band mean under 0.6 ms between halves; the short-sleep penalty holds at every age, while the long-sleep HRV penalty is flat under 30 and grows with age, largest in men aged 40 to 49 (HRV running 43.0, 40.6, 41.6, 41.4, 39.4 ms). The framing is associational, and per-member median sleep smooths over single bad nights, so read the band-level numbers as cohort averages.
Members who habitually sleep under 7 hours carry a real overnight recovery cost, visible in lower HRV and higher resting heart rate the next night; past 9 hours the cost is small and surfaces only on the most sensitive marker. The U-shape that has held in mortality epidemiology for fifteen years is visible night by night, in a single Ring cohort larger than most individual studies in that meta-analysis.
- Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep, 2010. PMID: 20469800.
- Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European Heart Journal, 2011. PMID: 21300732.
- Hirshkowitz M, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health, 2015. PMID: 29073398.
More bytes
Keep exploring

Across 230,179 Ring members, the dominant age change in sleep is more time awake at night, not less deep sleep

Time in target holds until the diabetic line, then collapses, across 1,169 members
